Mobile Medic Boosts Combat Casualty Treatment


The U.S. Army’s transition to preparing for large-scale combat operations has highlighted a capability gap in medical care delivery. Mobile Medic offers a telehealth solution to address this capability gap. By employing telecommunications technology, the tool is the tip of the spear for the Defense Health Agency and Medical Command’s virtual health line of effort.
In the contested environment of peer-to-peer conflict, units may lack the freedom of movement experienced during the recent stages of operations in Iraq and Afghanistan. Consequently, the ability to array forces on the battlefield will be limited. These mobility restrictions will affect specialized low-density health care providers. The inability to deliver support at the front lines threatens timely combat casualty care.
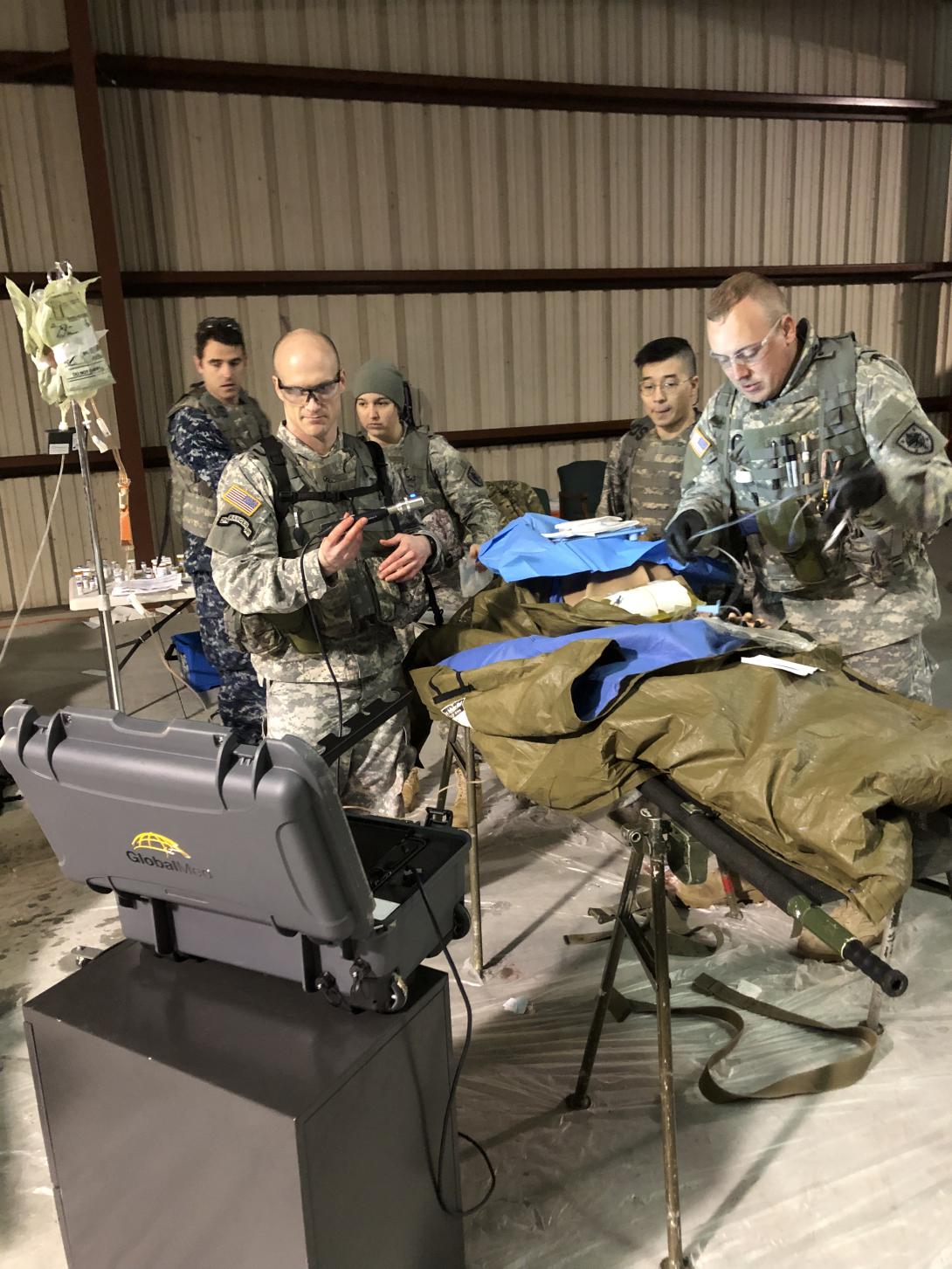
The Mobile Medic telehealth solution comprises a mobile and ruggedized computer system that facilitates video and audio feeds between forward locations and geographically separated, typically rear-based medical providers. It includes devices such as a stethoscope and electrocardiogram leads that transmit data across long distances.
Mobile Medic offers a potential equipment-based solution to facilitate health care delivery during large-scale combat operations. It allows tertiary care center specialists to provide point-of-care recommendations to the forward medics at the bedsides of sick and injured soldiers. These consultations can optimize casualty care while potentially reducing requirements to physically transport personnel to higher levels of care, accelerating the rate at which soldiers return to duty.
Previous National Training Center (NTC) rotations have featured use of the Mobile Medic device. The 3rd Armored Brigade Combat Team (ABCT), 4th Infantry Division, utilized it at the NTC in October 2018; the 2nd ABCT was used by the 1st Armored Division at the NTC in March 2019.
Using Mobile Medic equipment during these rotations helped solidify the potential utility of these devices during near-peer force-on-force conflicts; however, these rotations utilized wireless Internet devices connected to commercial cellular networks to establish connectivity between the Mobile Medic and rear locations. Commanders would benefit from the availability of alternative communications mechanisms for leveraging telehealth technology in the event that wireless devices are unavailable or experience jamming.
During the Joint Readiness Training Center (JRTC) rotation 20-02, the 2nd Infantry Brigade Combat Team (BCT), 4th Infantry Division, under the leadership of Col. Scott P. Knight, USA, brigade commander, became the first unit to successfully transmit an audio and video feed with Mobile Medic using tactical satellite communications systems during a combat training center rotation.
The use of Mobile Medic at the JRTC represents an important milestone in the development of battlefield telehealth technology. It provides proof of concept that BCTs may utilize this technology using their organic tactical communications modalities. This highlights the potential value of this device in the kinetic setting of large-scale combat operations.
The soldiers used the Transportable Exam Station (TES) Extreme Mobile Medic device. This military-grade tablet platform and impact-resistant casing can store myriad medical equipment, including a stethoscope, exam cameras, ultrasound devices, blood pressure cuffs and electrocardiogram leads. The Telehealth in a Bag (THIAB) device is a less comprehensive variation of the TES and includes a mobile laptop and peripheral medical devices. Although the team did not use the THIAB during training operations at the JRTC, an equipped THIAB was available at the JRTC Aid Station Rear.
Col. Knight’s team used the Warfighter Information Network–Tactical (WIN-T) Increment 2 Tactical Communications Node (TCN). Via this platform, the team successfully executed Cisco Jabber video calls from the field at the JRTC to the JRTC Aid Station Rear located at North Fort Polk and Baynes Jones Army Community Hospital. It also executed two calls to its home station military treatment facility, Evans Army Community Hospital (EACH), at Fort Carson, Colorado. Each of these calls lasted approximately five minutes with sustained high-quality video and audio feeds.
The methodology used to execute these calls was simple and readily replicable by BCT signal staffs. Using the WIN-T Increment 2 TCN, the team first ensured that the nonsecure Internal protocol router network (NIPRNet) enclave had a functioning Dynamic Host Configuration Protocol (DHCP) server setup in the router. Next, it consoled into the NIPRNet Tier 2 router and accessed the NIPRNet Tier 2 switch module either using a network virtual terminal protocol or secure shell commands. The team utilized any spare port not in use and ensured it was set up as an access port for virtual local area networks 58 and 59 modeled after a typical user access port.
The team opened the network and Internet settings on the Mobile Medic tablet, and then selected the option to Change Adapter. Generally, there are multiple adapters, including Ethernet and wireless. The Mobile Medic device pulls its own Internet protocol (IP) address; in its normal configuration, it tries to use the wireless adaptor and a Verizon Jetpack mobile wireless network device. To prevent this, the BCT disabled the wireless adapter and powered off the Verizon Jetpack. The team then plugged an Ethernet cable from the configured NIPRNet port on the TCN into the rear of the Mobile Medic. Taking note of which adapter was subsequently connected, the team right clicked on that adapter and selected Properties, and then double-clicked on Transmission Control Protocol/IP version 4.
If a DHCP server is configured, users select the option to pull an IP address automatically. If DHCP didn’t exist, the BCT gave the device a static IP based on the unit tactical template, ensuring use of a firewall as the default gateway.
Overall, the BCT signal staff emphasized the importance of not overthinking the Mobile Medic system. Mobile Medic is in essence a simple end user device analogous to any other NIPRNet computer added to the network.
The team conducted additional testing during reception, staging, onward movement and integration operations, including tests of the Mobile Medic device on a very small aperture terminal and the Combat Service Support Automated Information Systems Interface platforms. It connected the device wirelessly to these platforms, which required no IP configuration or port protocol and successfully executed approximately 20 calls. However, this platform was not used during force-on-force operations during the rotation.
The brigade learned several lessons during this testing. Support from telehealth experts based at military treatment facilities is critical. The unit received its Mobile Medic devices via sub-hand receipt from telehealth personnel assigned to the home station military treatment facility who traveled on temporary duty to Fort Polk, Louisiana. Initial equipment receipt occurred during reception, staging, onward movement and integration operations. This allowed the BCT signal staff to become familiar with the operation and troubleshooting of the device during initial communications exercises prior to initiation of force-on-force operations.
The familiarization of medics and providers is equally important to ensure they are comfortable with the operation of the device and buy into its use. In the case of the BCT, the medical and communications personnel utilized the device during multiple field exercises leading up to the JRTC 20-02; this prior experience was instrumental to the success of the work.
BCT staffs also must carefully consider both the resources the Mobile Medic requires and the opportunities it offers in determining how to incorporate use of this device into the battle rhythm. Like any video teleconferencing platform, this device has certain bandwidth requirements, in this case 450 Kbps to 1.3 Mbps. This may decrease the bandwidth for other warfighting functions if used during active operations.
When adding this device to the network, the bandwidth divides evenly among all users. Consequently, the Mobile Medic device only gets as much bandwidth as the Medical Communications for Combat Casualty Care, or MC4, computer used to send and receive emails. Moreover, the principal medical utility of the device does not lie in augmentation of tactical combat casualty care, which normally occurs when tactical communication system bandwidth is limited and treatments are time sensitive and sufficiently straightforward to limit the device’s value. Rather, the medics and providers maximized the utility of the device when using it to guide routine sick call operations in between kinetic operations to optimize care for routine and priority patients.
The unpredictable and chaotic nature of large-scale combat operations in particular may mean that the ideal time windows for use of this device change daily. Nevertheless, reserving use of this device to these time periods ensures minimal impact on communications needed for combat operations while offering fewer disruptions to patient care activities. Medical providers on the battlefield can take the requisite time and resources to tap into the expertise of rear-based health care specialists in making disposition decisions.
The greatest impact of Mobile Medic comes not necessarily from optimization of treatment decisions but rather from preservation of combat power through minimization of the transfer of soldiers with less severe illnesses and injuries to rear-based higher echelons of care. For example, traumatic brain injuries potentially represent one such instance that may not be imminently life threatening but might benefit from a remote neurology consultation to guide whether and when rearward transportation is necessary.
The examination of the Mobile Medic equipment during the JRTC rotation 20-02 only represents the beginning and much work remains. The hope is that future units may build upon the experience to further refine the methodologies for use of this device in both training and combat operations.
Future exercises also would benefit from formal surveys of signal staffs and medical teams to ascertain additional thoughts about best practices related to incorporation into tactical networks, ideal timing per unit battle rhythm, the optimal number of devices each echelon can effectively use, and the best use and contributions to patient care activities.
It also will be important to ensure that units possess the necessary medical maintenance personnel and support to service this equipment. Line commanders will ultimately see in these experiences the opportunity for more widespread use of this technology to further advance the capabilities of their medical teams.
Maj. Michael D. April, USA, is a medical corps officer, emergency physician and brigade surgeon. Maj. Daniel P. Brady, USA, is an engineer officer and brigade executive officer. Both serve with the 2nd Infantry Brigade Combat Team, 4th Infantry Division.



Comments